Question 3. What factors are associated with message receptivity and behavioral compliance?
The literature shows consistency on message development processes and key variables influencing behaviors.
Receptivity of messages requires that communication is relevant, clear, understandable, and delivered through trusted and commonly accessed channels and sources (Lin et al., 2016). Persuasive messages are more effective in motivating individuals to comply than fear-based messages, especially when messages are not tailored at the individual level (Liu et al., 2017). Building and maintaining trust is vital to the effectiveness of communication but it can be weakened by message delivery, content, individual experiences with public health emergencies, and individual beliefs and values. Targeting messages, delivery channels, and message source to population segments is important (Hoda, 2015; Hou et al., 2018) Individual responses to communication are shaped by an interaction of personal, contextual and cognitive factors and it is extremely important to identify them and incorporate such information into communication, including who delivers the message (Vaughan & Tinker, 2009). Understanding local needs for communication and using those insights to design messages and select messengers and channels is associated with improved behavioral compliance (Holmes et al., 2009; Lin et al., 2014; Novak et al., 2019; World Health Organization, 2018). This is also relevant as the pandemic progresses and measures change, as trust in sources, especially government, changes throughout the crisis as well as willingness to adhere to measures (Henrich & Holmes, 2011; Lachlan et al., 2014). Communicating uncertainty about aspects of public health emergencies to the public helped to reduce uncertainty about protective behaviors and minimized the damaging effects of misinformation.
Key variables associated with behavioral compliance to protective measures include: trust, risk perception, perception of responsibility to contribute as an individual to a community problem, perceived disease severity, information seeking, level of worry, knowledge about the disease, self-efficacy, timing, transparency, exposure to credible media sources, and experience with a pandemic (Bults et al., 2011; Cordova-Villalobos et al., 2017; de Zwart et al., 2009; Holmes et al., 2009; Hou et al., 2018; Lin et al., 2014, 2016; Maduz et al., 2019).
Trust includes: in public officials, that the source is credible, that the promoted measure will achieve the results (i.e., outcome expectancy), and that they can perform the behavior (self-efficacy). For example, Hou et al., 2018 found “during the outbreak of SARS, knowledge level on the disease itself was not associated with adoption of preventive measure but public trust was.”. In the Dutch study of Bults et al 2011, self-efficacy (trust in one’s self) was the largest predictor variable. Sharing of personal data (such as needed for digital or classical contact tracing), predictors include a sense of social duty, having some self-benefit and understanding the public good is being served (Skatova & Goulding, 2019). Public trust in science and public health authorities also promotes data sharing (Aitken et al., 2016).
The underlying and overarching focus of communications and actions must illustrate the necessity of collective action to contain SARS-CoV-2. This crisis can only be solved together, as a community and society. Each person in Switzerland is part of the social tissue that makes this country what it is. Communication needs to remind people and firms of this stressing the actions help both self and others needed to contain the virus, and thus keep health, economy, and society prosperous.
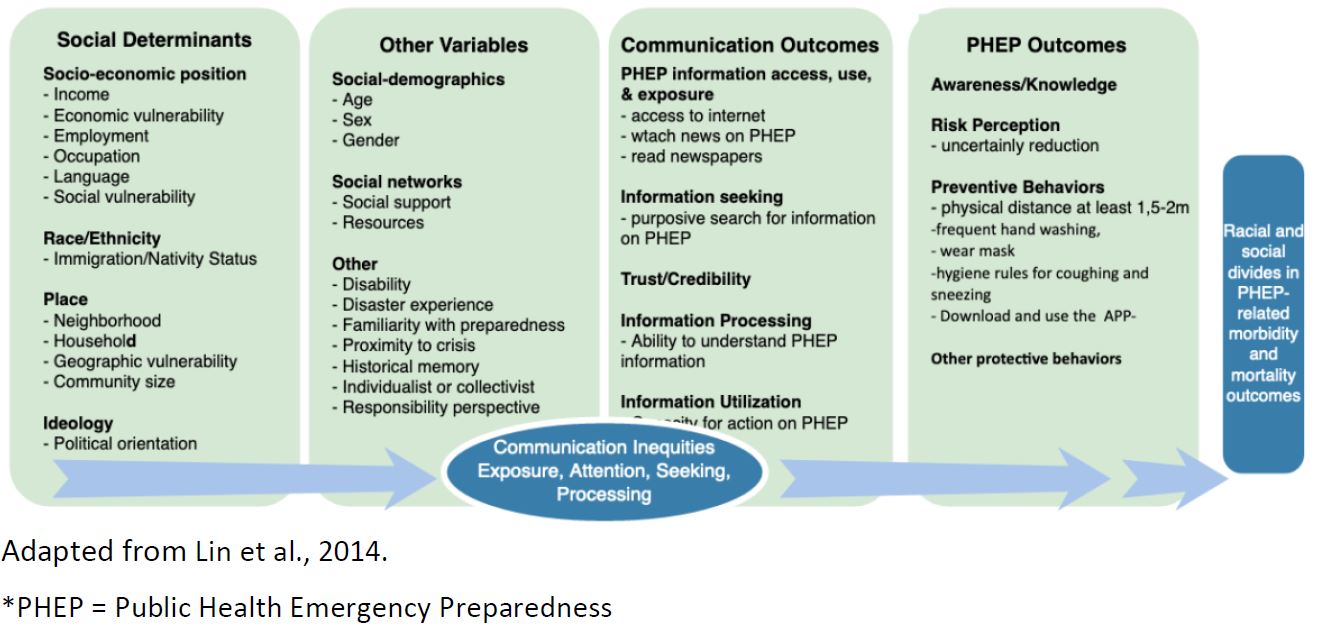
Social determinants of health behavior and communication accessibility are associated with behavioral compliance (M. Lee et al., 2019; Lin et al., 2014). Lower socio-economic status is associated with knowledge of health emergency (Hou et al., 2018) and “lower levels of awareness and knowledge regarding pandemics, leading to poorer behavioral responses when dealing with an outbreak” (Lin et al., 2016). Further, “social and individual determinants (i.e. education, income, race/ethnicity) may lead to inequalities in individual or group-specific exposure to public health communication messages, and in the capacity to access, process, and act upon the information received by specific sub-groups- a concept defined as communication inequalities”. (Lin et al., 2014). Thus, communication must be pushed to people where they are, rather than relying on pull mechanisms.
Channels of communication need to reflect what all people in Switzerland use and trust for SARS-CoV-2 related information; which means TV, radio, and newspapers, which are perhaps the most important channels of information during emergency situations (Holmes et al., 2009; Hou et al., 2018; Jardine et al., 2015; Lin et al., 2014; Sjöberg, 2018). Other channels matter, but are often secondary in pandemic situations. For example, the nationally representative online survey in Switzerland (N=758) during 2017, ICT sources were preferred by 32% of the sample although 86% indicated that they used official information sources for information. (Maduz et al., 2019).
In summary: To increase compliance with recommended protection measures the evidence suggests:
- Provide clear, consistent, understandable, actionable, trustworthy information that buildsself-efficacy and responsibility of the target audience and that is accessible and done sothrough mass media sources and well as social and online channels used by target audiences
- Segment and target audiences for communication. One size messaging will not fit all;targeting and tailoring are key
- Focus on mass public, but also targeted communications for those behaving sub-optimally orat higher risk of infection by using messages that resonate and messengers that are trusted byeach target population
- Listen to people and react accordingly. Engage in two-way communication so that messagesand measures reflect the reality of all population groups. This includes listening to needs andconcerns and using this to inform communication messages and delivery options. Peoplemust know and believe that they are being “heard” regarding all of their challenges caused bySARS-CoV-2, beyond the threat of infection.
- To build trust and self-efficacy, show and explain “how to do” and that all can contribute andnot only “what to do” and “why it matters” (pros and cons).
- Also to build trust, policy and public health must take the broader societal implications of theepidemic and the restrictions very seriously.
- Highlight the benefit to self and others.
- Utilize traditional channels, including TV and newspapers, to communicate
- Approach communication from an egalitarian basis, and thus make efforts to reachpopulations who are allophones, less connected online, or disabled.
- Increase accessibility of communications delivered to the mass public, such as including sign-language in press conferences, TV adverts, online videos, and making materials accessible fordifferently abled persons, people with low literacy, low vision, low hearing, who speak non-Swiss languages.
- Do not take for granted that the public understands and believes the message. Pretestmessages with target groups
- As measures change, what remains important must be stressed, not just what is new
- Congratulate and thank the population for the what they have accomplished together, asconcretely as possible (what actions they did with what benefit) without conveying it is ok torelax protective behaviors.