Question 1. What are the identified risk factors for hospitalization in patients with SARS-CoV-2 infection?
Introductory note: Hospitalizations for COVID-19 can be grouped into 4 categories: 1) medical reasons as direct consequence of SARS-CoV-2; 2) medical/social reasons, but not directly associated to SARS-CoV-2 , e.g. elderly patient not able to care for him/herself; 3) patients or physician-related causes: fear of the disease, or potential for adverse outcome, but no clinical necessity, and 4) for reasons of isolation or cohorting patients, without clinical necessity.
This review will focus on group 1, which is largest group in Switzerland. The hospitalization rate of SARS-CoV-2 infection is highly variable around the worldm depending on the structure of the population and the organization of the healthcare system. A modelling study from France suggests that around 3.6% of infected individuals are hospitalized (95% CrI: 2.1–5.6) (Salje). Since March 2020, 7.3 % of confirmed infections lead to an hospital admission in Switzerland (FOPH) :

Many risk factors associated with hospital admission have been described (Salje – Guan – Richardson – Zhou – Petrelli):
- increasing age, with no specific limit (Salje – CDC – Lewnard – Petrelli)
- male gender (RR 1.25, 95% CrI: 1.22–1.29) (Salje)
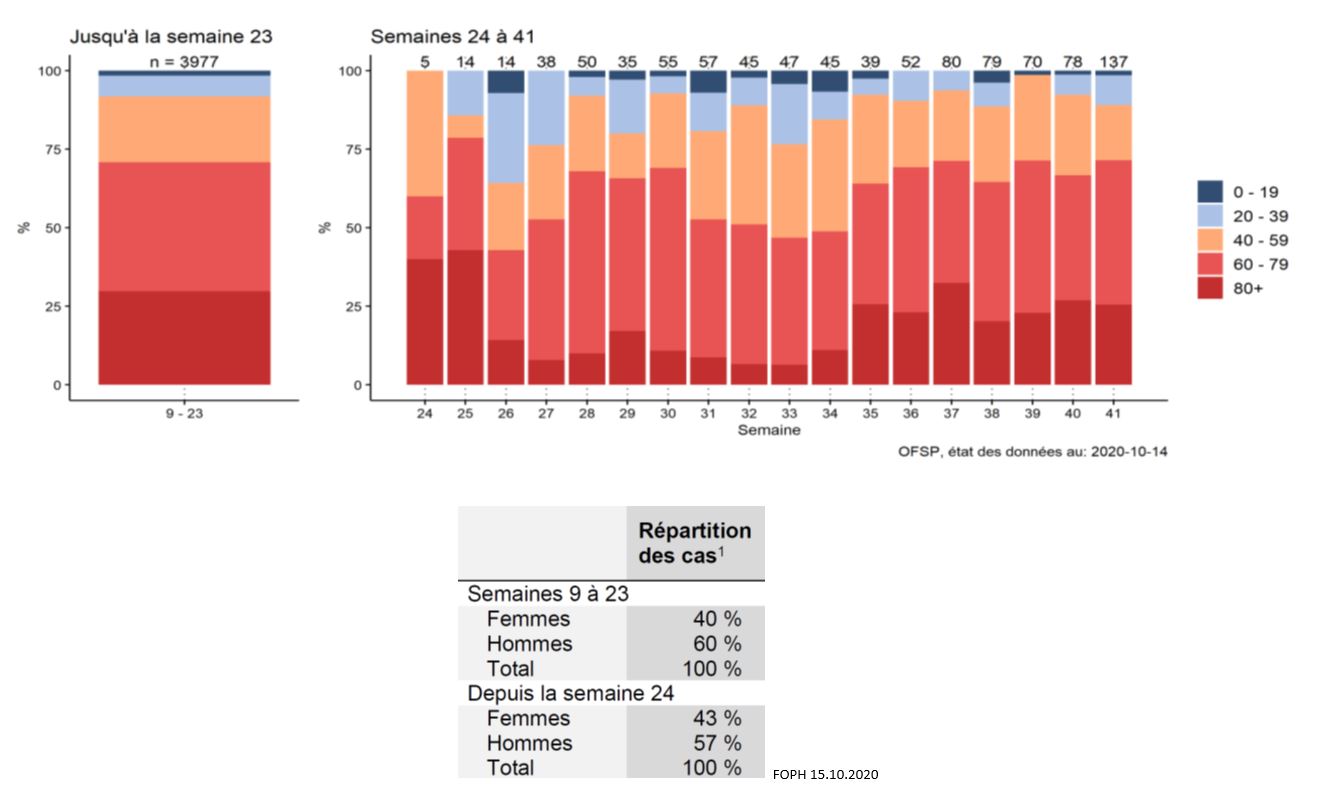
These data are concordant with the age and sex distribution of hospitalized patients in Switzerland (FOPH 15.10.2020) :
Comorbidities :
- hypertension and cardiovascular diseases (arrhythmia, heart failure, ischemic heart disease, chronic kidney disease) (Petrelli)
- obesity is associated with a 2.13 increased risk (Popkin)
- chronic respiratory disease, particularly COPD (RR 1.88, 95% CI, 1.4–2.4) (Alqahtani).
- diabetes
- smoking (RR 1.45, 95% CI: 1.03–2.04) (Alqahtani).
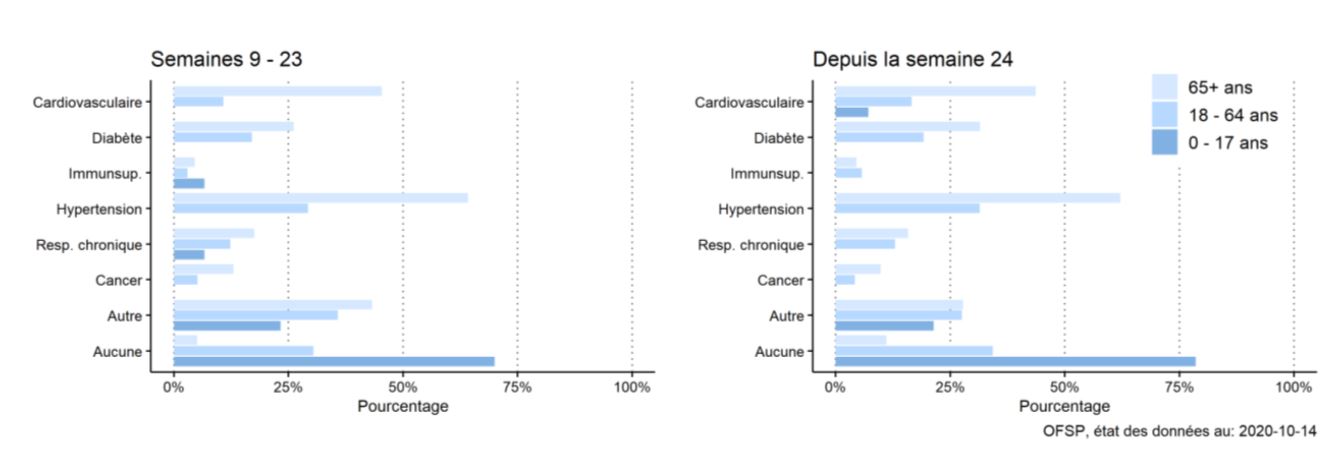
These risk factors are intertwined and sometimes merely associated with age. But, comorbidities are present in over 80 % of hospitalized patients in Switzerland, which is concordant with the published literature (Salive) :
Some prognosis model have been published, but without external validation, limiting their use (Wynants).
An on-line calculator is available (https://riskcalc.org/COVID19Hospitalization/), but has not been validated for Swiss patients (Jehli)
Uncertainty: The risk of an adverse outcome and hospitalization increases with age, male sex, obesity, and with the number of cardiovascular and pulmonary co-morbidities. The risk increase is gradual and additional factors such as host response, inoculum, genetic factors, and others may play a role on the individual level. No validated evaluation tool is available for the Swiss population to identify patients at high risk who may benefit from a preemptive of prophylactic therapy.
Question 3. What are the identified risk factors for mortality in patients with SARS-CoV-2 infection?
Introductory note: General mortality (case fatality) is estimated between 0.7 and 3.6 % (CEBM – Williamson – Verity), and the Infection Fatality Ratio (IFR) that was estimated around 0.65-0.70% (Salje – Verity) is probably lower, around 0.27 according to the WHO (Ioannidis). In Switzerland, the mortality of confirmed cases is 2.4 % at this stage. The mortality rate of hospitalized patients was initially estimated around 18.1% (95% CI: 17.8–18.4) (Salje), but is probably closer to 7%, according to a recent meta-analysis (Grant). ICU mortality varies very much and is reported to be 37 % in the US (Gupta) and 45 % in Lombardy (Grasselli 2), and around 24% in a recent registry including Swiss patients (Wendel-Garcia). The mortality in nursing home resident is probably around 35%.
Positive results of clinical trial could modify the therapy and influence the mortality rate and the associated risk.
Many factors associated with a higher mortality have been identified :
Factors associated with mortality in the general population (CDC 2020):
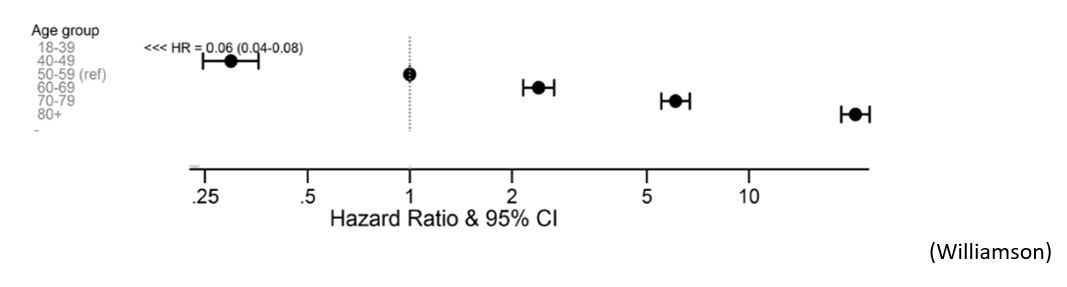
- Age is clearly associated with an increased risk the risk of dying (Knight – Lewnard – Petrelli – Williamson), from 0.001% under 20 to 10.1% over 80 (Salje).
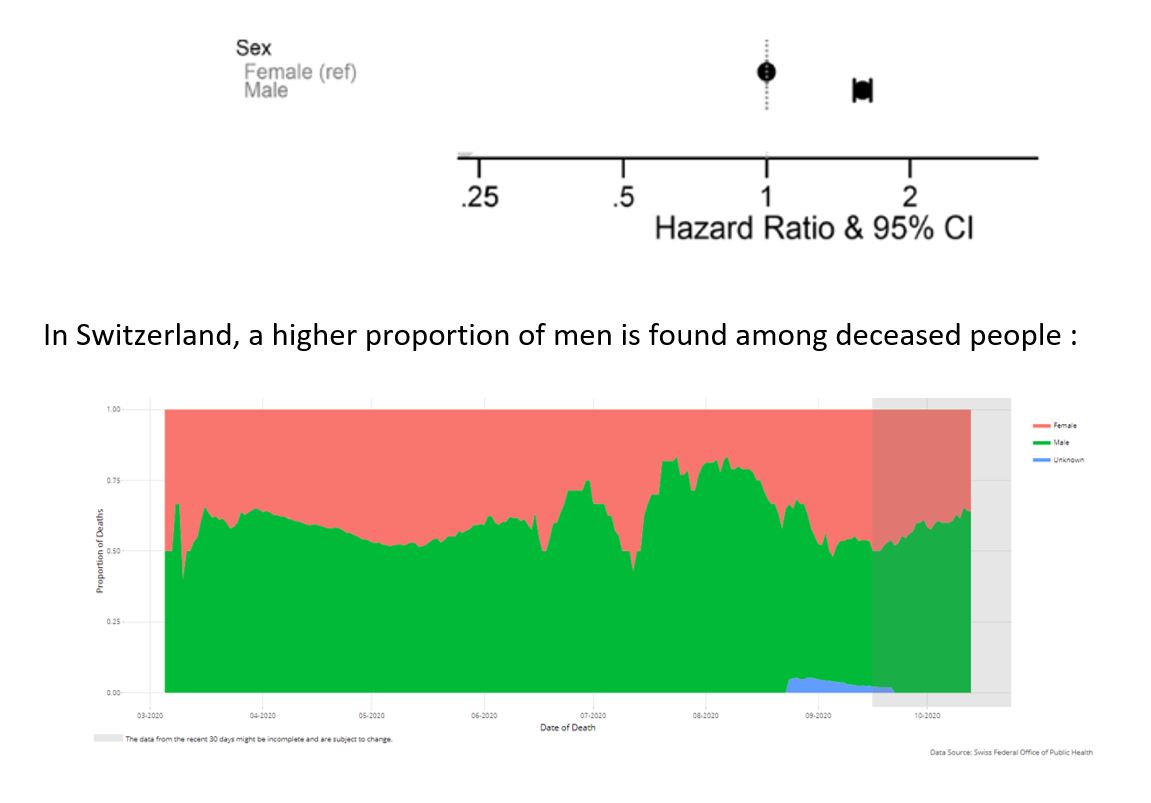
- male sex (Salje – Williamson) :
- Other factors associated with mortality :
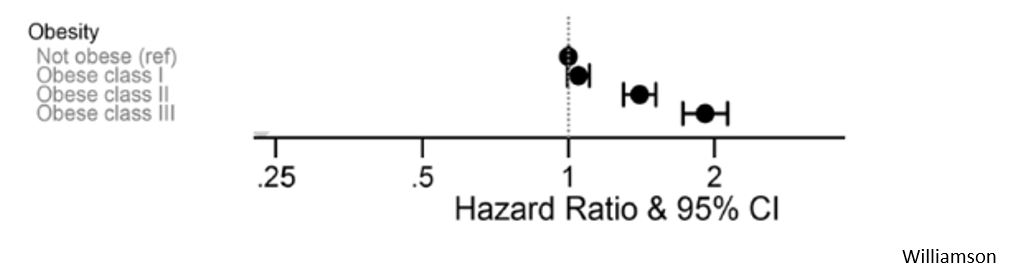
- obesity is associated with a 48 % increased risk of dying (Popkin -Williamson)
- comorbid conditions (CDC – Williamson), particularly :
- heart failure (Petrelli)
- dementia
- chronic liver disease
- diabetes (Petrelli – Williamson)
- nursing home residency (CDC)
- chronic immunosuppression (Williamson)
- cancer (Petrelli – Williamson)
- comorbid conditions (CDC – Williamson), particularly :
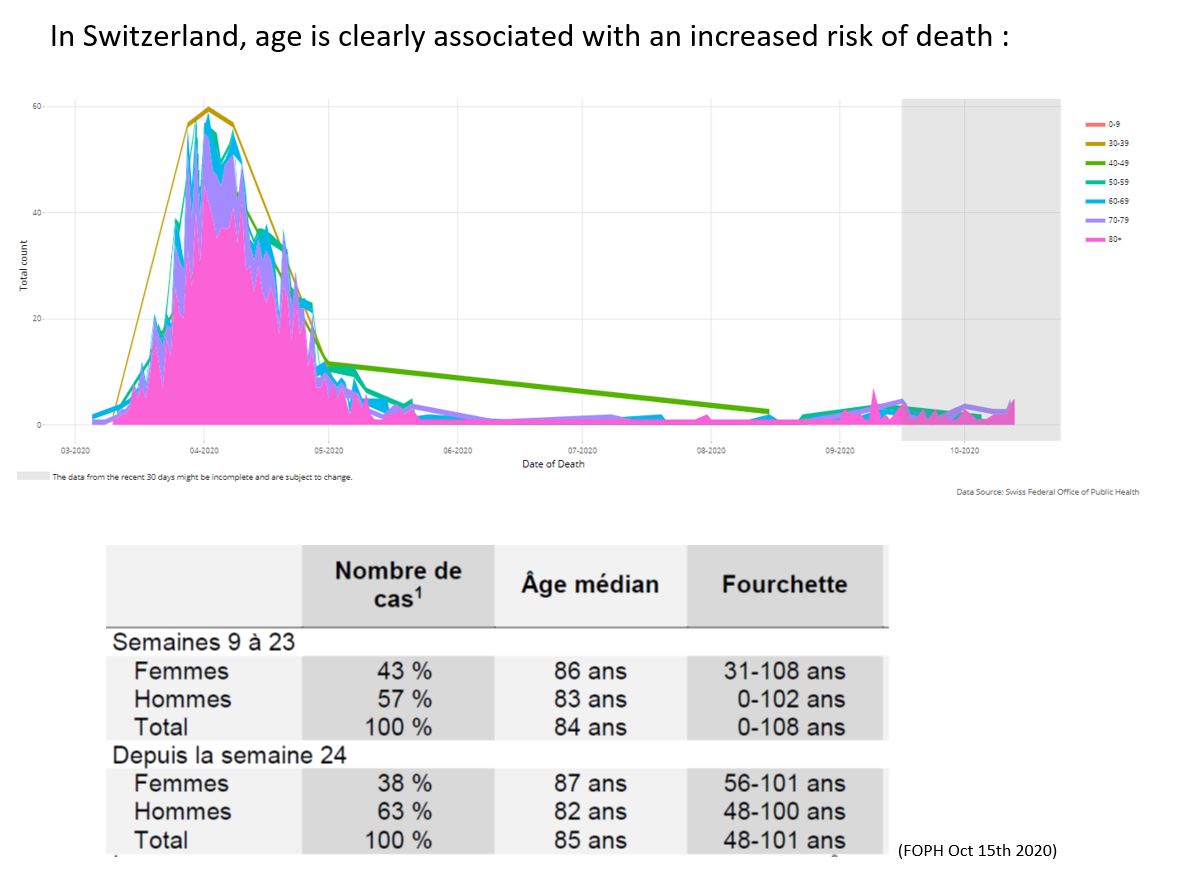
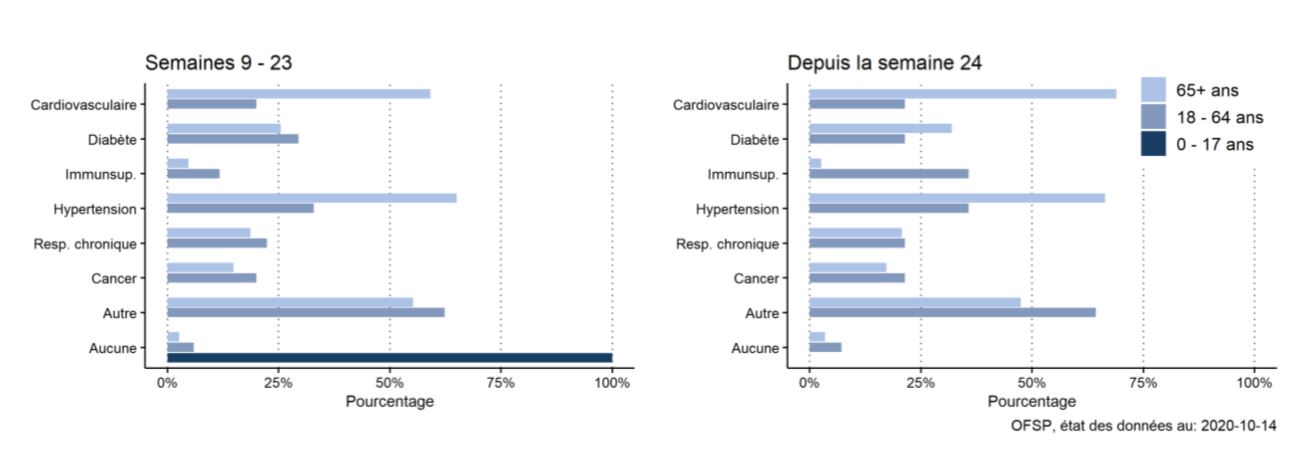
In Switzerland, the majority of deceased patient had at least one comorbitidy, in accordance with these data :
Factors NOT associated with mortality in the population (Reynolds):
- antihypertensive treatment, including ACE inhibitors and angiotensin-receptor blockers (Mackey)
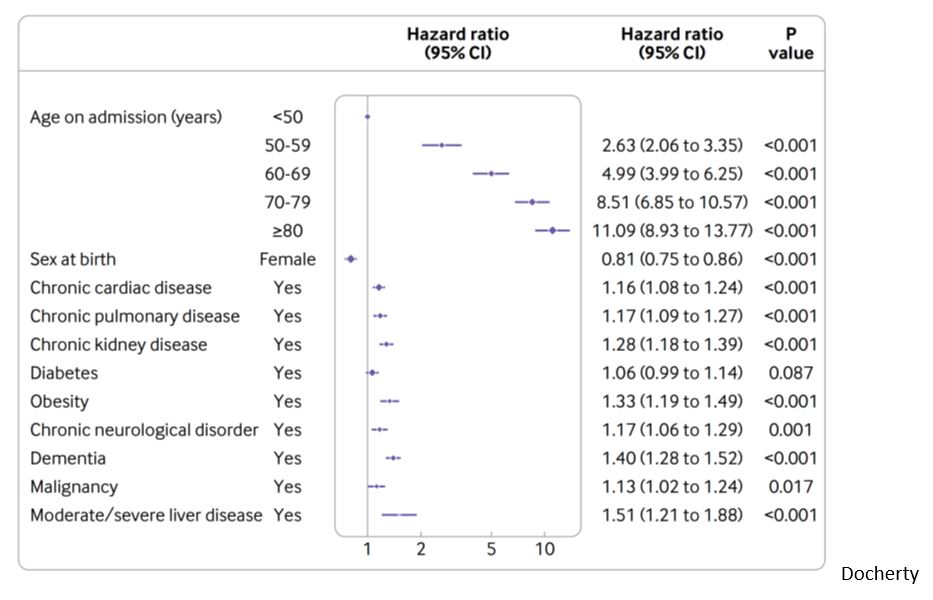
Independent factors associated with mortality in hospitalized patients (Liu – Ruan – Docherty):
- increasing age, starting from 50 year old
- sex: female sex is associated with decrease mortality : HR 0.81 (CI 0.75 to 0.86) (Docherty – Knight)
- coronary artery disease : OR 2.70 (95% CI 2.08 – 3.51)
- heart failure : OR 2.48 (95% CI 1.62 – 3.79)
- cardiac arrhythmia : OR 1.95 (95% CI 1.33 – 2.86)
- COPD : OR 2.96 (95% CI 2.00 – 4.40)
- current smoking : OR 1.79 (95% CI 1.29 to 2.47)
- smoking and COPD have also been associated with increased mortality in a meta-analysis (Alqahtani)
- obesity (Docherty)
Factor NOT associated with mortality in hospitalized patients (Mancia – Reynolds – Zhang P):
- antihypertensive treatment, including ACE inhibitors and angiotensin-receptor blockers
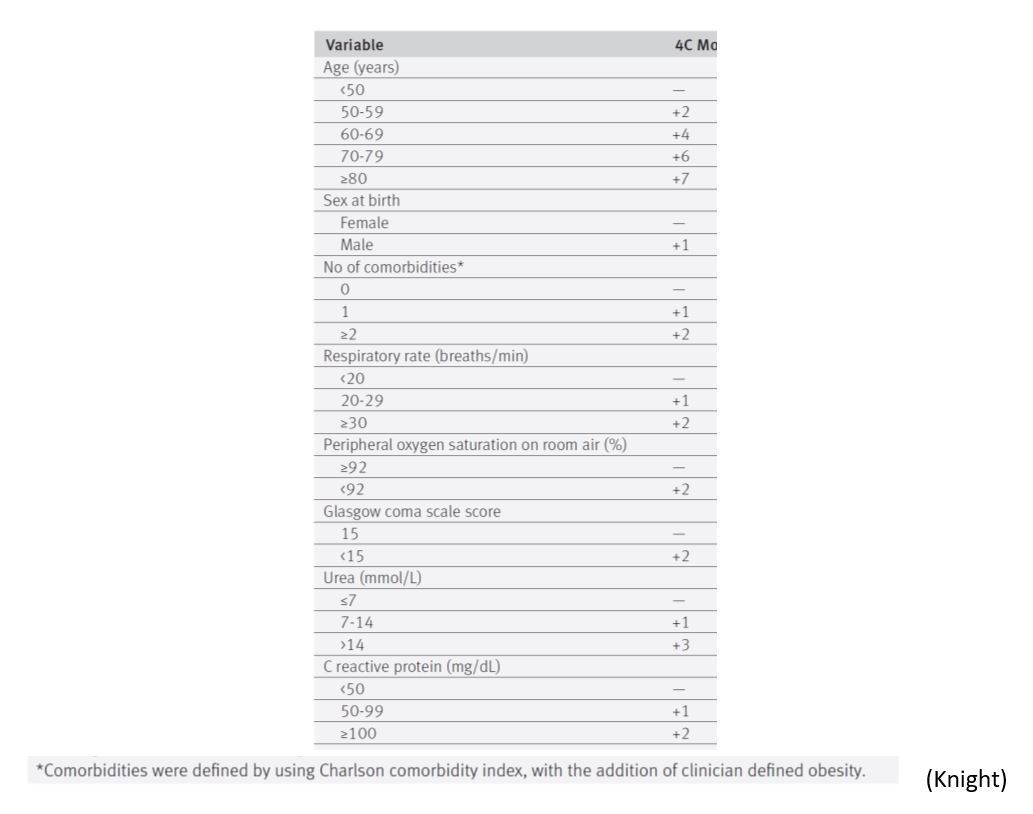
The 4C Mortality Score proposed by the WHO, based on the ISARIC cohort, is a risk stratification model for the prediction of death in hospitalized patients (Knight). It categorises patients in low, intermediate, high, or very high risk of death, based on easy-to-obtain parameters, but it has not been validated for Swiss patients:
Factors associated with mortality in the ICU:
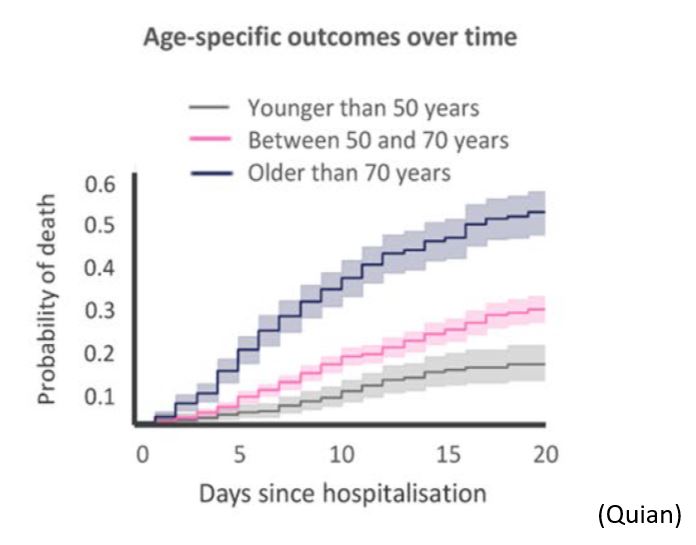
- age is associated with ICU mortality (CDC – Qian – Grasselli 2 – Gupta), as an independent factor, with an hazard ratio of 1.75 (95% CI, 1.60-1.92) (Grasselli 2), and an OR of 11.15 (95%CI, 6.19-20.06) for over 80 years vs less than 40 (Gupta).
- acute respiratory distress syndrome (ARDS) and sepsis reported in 100 % of dying ICU COVID-19 patients (Chen)
- male sex (HR1.57; 95%CI, 1.31-1.88), high oxygen (HR, 1.14; 95%CI, 1.10-1.19) and PEEP (HR, 1.04; 95%CI, 1.01-1.06) need, low PaO2:FiO2 ratio (HR, 0.80; 95%CI, 0.74-0.87) on ICU admission are independently associated with ICU mortality (Grasselli 2 – Gupta)
- history of chronic obstructive pulmonary disease (HR, 1.68; 95%CI, 1.28-2.19), hypercholesterolemia (HR, 1.25; 95%CI, 1.02-1.52), and type 2 diabetes (HR, 1.18; 95%CI, 1.01-1.39), higher body mass index (>40 vs <25: OR, 1.51; 95%CI, 1.01-2.25), and active cancer (OR, 2.15; 95%CI, 1.35-3.43) are also independently associated with higher mortality (Grasselli 2 – Gupta)
- no validated prediction models has been validated, as they were derived from small cohorts of selected patients, with a high risk of bias, no or poor external validation (Wynants)
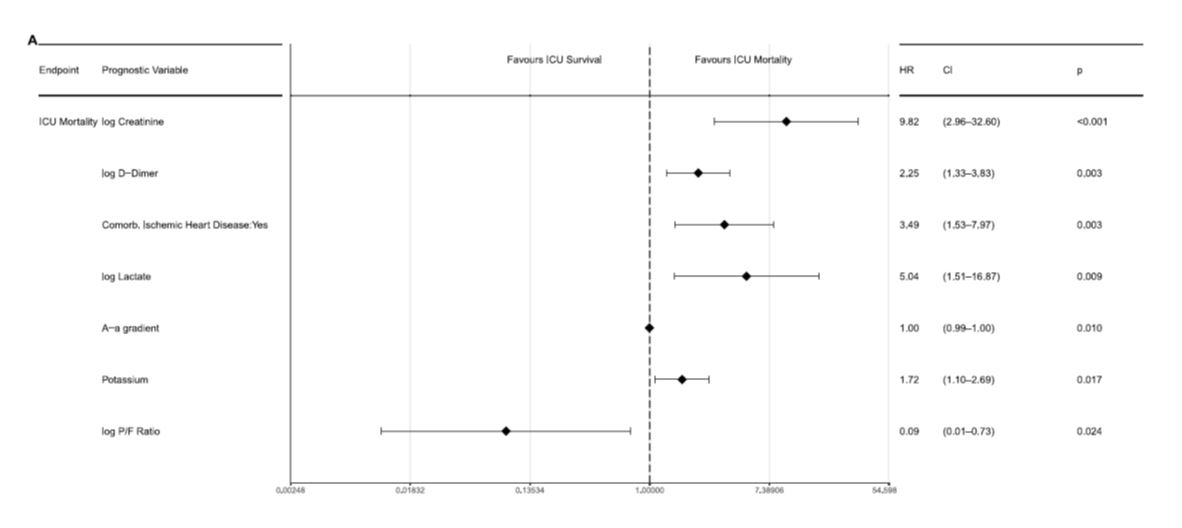
- data from patients admitted to the ICU in Switzerland (Wendel-Garcia) show that very few factors are independently associated with the risk of dying:
Uncertainty: reported death rates are highly variable, depending on the country, the type of patients included (general population, nursing home residents, ICU patients). Therefore, mortality data must be interpreted with caution. The total incidence and prevalence of infected patients in the population is unknown, mortality data have often been published early on the course of the pandemic (Baud), and death certificate do not always differentiate COVID-19 -related or non COVID-19 -related death. Definite and reproducible data on mortality will probably be available in the aftermath of the pandemic. In the meantime, age, male sex and co-morbid conditions are clearly associated with an increased risk of dying. As already mentioned, therapies with proven efficacy could modify the mortality and associated risks